Expanding health access in rural communities through telehealth in schools

Dr. Steve North initially bypassed medical school to join one of the first Teach for America (TFA) cohorts, but his experience teaching in rural North Carolina ultimately led him on a path straight back to medicine.
Through TFA, Dr. North was assigned to Edgecombe County, where he taught exceptional children in fifth through eighth grade. One day in class he noticed a student resting his head on a desk. The student had injured himself at home, stepping on a nail that was protruding from a floorboard. The injury wasn’t serious, but did need medical attention. The child’s family was enrolled in Medicaid and wanted to take him to see a doctor. The problem was they did not have access to transportation.
Dr. North reached out to his student’s family and volunteered to take him to the doctor. They eagerly accepted his offer. That trip to the doctor’s office is when he saw firsthand the discrimination Black kids with Medicaid cards sometimes face. He decided to become an adolescent medicine specialist at the conclusion of his time with TFA to help provide medical care to the kids who have the hardest time accessing it.
During his time in medical school in the 1990s, Dr. North learned about both school health centers and telehealth. In 2010, he combined everything he learned to establish the Center for Rural Health Innovation (CRHI) in Spruce Pine. CRHI now utilizes telehealth to operate 108 Health-e-Schools school health centers (SHCs) across all regions of North Carolina with a focus on equity and equitable access.
As with most SHC operators, the goals of CRHI are to make health services more accessible to students and to reduce the amount of time students have to spend out of the classroom receiving medical care. The telehealth model is ideal on both fronts.
When students at schools with traditional SHCs feel sick, they can request a medical visit. The student would then leave the classroom to be examined by a physician assistant or family nurse practitioner at the on-site SHC. The clinician would provide appropriate treatment, typically enabling the student to return to class. Without an SHC, students either go without medical care or miss more essential class time by being removed from school for a medical visit off-site.
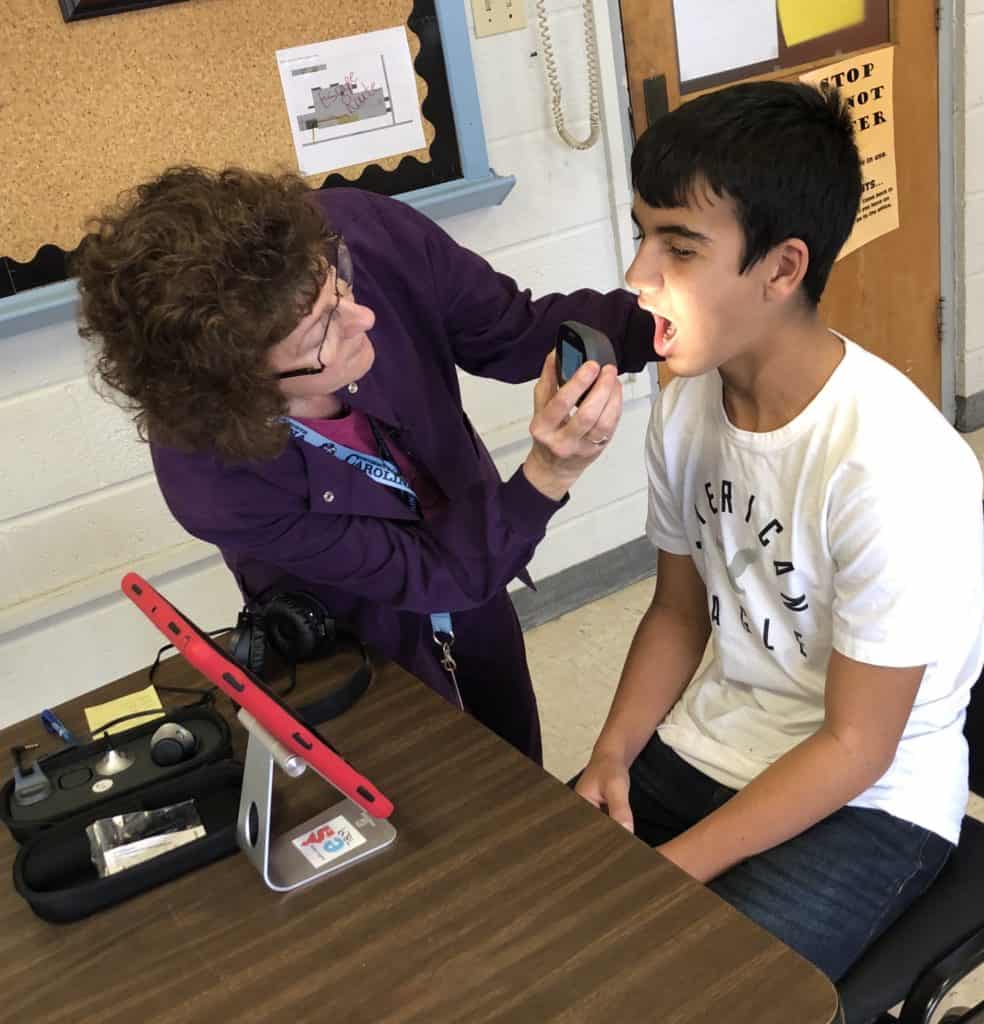
For students to participate in the Health-e-Schools program, the process is similar. The SHCs operated by CRHI don’t have on-site clinics operating on school campuses. Instead, one or more staff members at a school are trained to use a telehealth unit – CRHI uses a TytoCare model – which connects the student to a licensed clinician.
The staff member, often a school nurse, can do this from a designated office or an otherwise empty classroom anywhere on campus. This means the overhead and startup costs are significantly lower than they would be for establishing a traditional SHC. The cost of a telehealth unit is currently around $2,500 compared to the tens of thousands of dollars it can cost to outfit a full SHC facility.
Because school nurses often serve multiple schools and thus are not available at every school every day, any adult at a school can be trained to use the telehealth equipment to facilitate a Health-e-Schools consultation. This system expands access to care for students and keeps them in school.
Health-e-Schools is also available for use by staff members. Executive Director Amanda Martin explains, “The practical reason for that is if one child misses one school day, that’s one. If one teacher misses one school day, that’s 20 to 30.”
For fiscal year 2019-2020, CRHI’s total budget was about $570,000. Around $410,000 of that came from grants, including those from charitable foundations, community health grants, and the North Carolina Department of Health and Human Services. CRHI also brings in about $77,000 from contracts with health departments in Duplin and Pender Counties. The center covers less than 10% of their costs through traditional medical billing, including Medicaid. The remainder of its funding comes from consulting fees. As Martin puts it, “It’s cool because I’m able to generate revenue to run my local program by talking about my local program!”
A major challenge in determining whether school-based health programs are beneficial is the inability to merge health data (protected by HIPAA) with educational data (protected by FERPA). This makes it almost impossible to show whether improved access to healthcare has an impact on student learning. CRHI has not had the financial means to pay a researcher to evaluate its program outcomes, so it has not yet sought permission from parents or guardians to merge these data.
The current coronavirus pandemic presents challenges and opportunities for CRHI. While the pandemic has increased the public’s familiarity and comfort with the concept of telehealth, it has also introduced new misunderstandings about the technology.
“I don’t have to justify telehealth or explain telehealth anymore. What I have to say is, ‘This is not Zoom health!” Because a Zoom appointment with your family doctor for an ingrown toenail is not what I’m talking about,” explains Martin.
The form of telehealth utilized by CRHI is not simply an audio or video call with a clinician. TytoCare units come with blood pressure cuffs and other integrated digital tools to examine ears, noses, throats, etc.
With more members of the public recognizing the utility of telehealth, there’s been greater demand for the consulting services offered by CRHI. It’s possible their model will shift more toward consulting as the pandemic continues and if students are kept out of school.
“We’re definitely more in demand for our knowledge and expertise and experience,” Martin said. “I could have talked to someone twice a week about how to set up a program over the last few months. I finally had to stop; I was just exhausted!” Now Martin just shares a link to a recorded webinar.
There’s also uncertainty about how Health-e-Schools will operate when students return to school this fall. The top diagnosis for students who utilize Health-e-Schools is upper respiratory illness. Under CDC guidelines for stopping the spread of COVID-19, students with upper respiratory symptoms would have to be isolated before being sent home. This presents a special challenge for SHCs without dedicated facilities.
One solution would be for Health-e-Schools to act as the conduit between students and their family doctors’ if schools close their door again during the 2020-2021 academic year. Doctors themselves are seeing the utility of telehealth, but may not have the time, skills, or resources to integrate it directly into their own practices. CHRI could serve as the middleman connecting doctors to kids.
CRHI already operates SHCs in 108 schools across North Carolina, and it continues to expand. It’s easy to add new locations because the cost of telehealth is so low.
“I want telehealth to be available to every kid in every county of North Carolina, but I don’t think CRHI should be doing that,” asserts Martin. “I think we need a more regional and local solution. There’s a beautiful formula for how to recreate our exact programs with tweaks for what we’ve learned along the way. Sharing that is an important part of our work.”
This article is part of a series on innovative approaches to health in schools. Find the rest of the articles here.